



MME stands for Morphine Milligram Equivalents. Because all narcotics are synthesized from opium, healthcare professionals have developed a formula that allows an easy conversion to be made to compare the doses of different narcotics.
With the increase in mortality associated to opioid overdoses, many government healthcare organizations have been steering large clinical studies to compare the association between higher doses of opioids and the risk of overdose and long-term side effects.
Per the Centers for Disease Control and Prevention (CDC), in a national sample of Veterans Health Administration patients with chronic pain receiving opioids from 2004-2009, patients who died of opioid overdose were prescribed an average of 98MME/day, while other patients were prescribed an average of 48MME/day.
What this means is when calculating the total daily dose of opioids of all the patients during that 5-year period, patients with an MME greater than 90 were at a greater risk of overdose. This does not suggest that all patients pain tolerance should be looked at the same, nor does it recommend that a patient must drop doses immediately to be within this range. What this does mean is patients with an MME this high may benefit from closer monitoring, reduction by tapering of opioids, alternative therapy, prescribing of Narcan, or any other means of reducing the risk of an overdose.
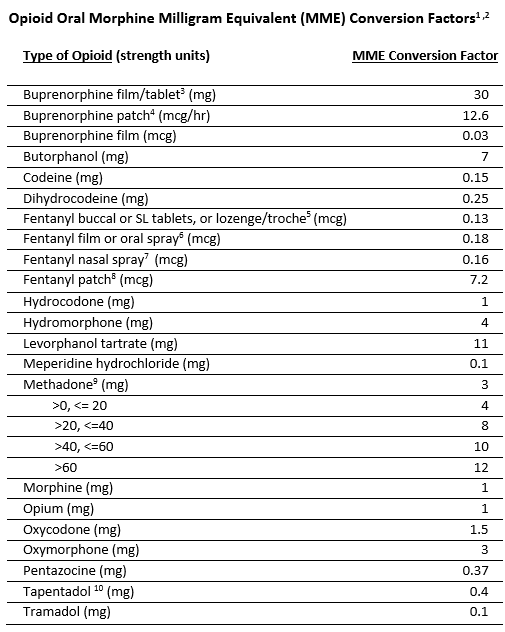
The CDC MME conversion factor to calculate Morphine Milligram Equivalents is 3. CMS uses this conversion factor when analyzing Medicare population opioid use. CMS uses the graduated methadone MME conversion factors to calculate MME within the Overutilization Monitoring System (OMS) for identifying and reporting potential opioid overutilizers.
Patients who use opioids should not look at this recommendation as anything negative. MME is being used to study trends in patients throughout the world and to better understand what doses have been causing more overdoses and risks. Unfortunately, pain management recommendations change so often that patients who have been on chronic opioids were started on pain treatment based off different recommendation. However, newer recommendations have proven that higher dosages haven’t been shown to reduce pain over the long term.
One randomized trial found no difference in pain or function between a more liberal opioid dose escalation strategy (with average final dosage 52 MME) and maintenance of current dosage (average final dosage 40 MME). What this means is that once the patient can taper down to a lower dose, the patient found no difference in pain versus building a tolerance at a higher dose.
In an effort to combat the opioid epidemic, IWP Pharmacists proactively reach out to patient’s providers with a high MME to determine if the provider is using caution when prescribing opioids and if the provider ensures that the patient is being properly monitored and has considered tapering of dosages. IWP has a standing order which allows a pharmacist to prescribe naloxone to any patient who requests it.

Our goal is to ensure patient safety while advocating for patient’s medication needs. By requesting additional documentation for patients on high doses of opioids from providers, IWP is improving the way opioids are prescribed, while ensuring patients have access to more effective pain management and reducing misuse, unwanted side effects, and overdose.