


Pharmacy Choice White Paper
INTRODUCTION
Managing workplace injury pain can be an arduous task for medical providers, patients, and researchers alike as the spectrum of treatment is complex, with several factors to consider for each patient. To accommodate individualized treatment, the field of pain management continues to expand access to non-pharmacological options and opioid alternatives while navigating the intricacies of state and federal regulatory environments. However, even as advances in the field are evolving, they can, at times, be limited in their capacity.
Non-opioid pharmacological options in workers’ compensation commonly include, but are not limited to non-steroidal anti-inflammatory drugs (NSAIDs, i.e. Motrin, Advil), dermatological agents (topicals such as creams, ointments, gels), acetaminophen (Tylenol), cortisone injections and gabapentinoids, which relieve pain for particular conditions in the nervous system. Whereas non-pharmacological options may comprise of physical therapy (PT), acupuncture, spinal cord stimulation, and electric signal therapy. PT is much more apparent in the workers' compensation space as a non-pharmacologic alternative with efficacy data more widely available.
Workplace injuries can happen in any industry, even for remote workers. Nevertheless, there are a few industries considered high risk where work-related injuries occur more often. Per the Bureau of Labor Statistics (i), these fields of work include construction, warehousing, transportation and various agricultural occupations. Although, industries may vary in their workplace injury occurrence, the top work injuries keeping workers off the job, according to the National Safety Council (ii), include:
a.) Sprain, strains, and tears
b.) Soreness and subsequent pain
c.) Cuts, lacerations, punctures
Common injuries resulting in lost workdays consist of:
a.) Overexertion (i.e. lifting, lowering, repetitive motion)
b.) Contact with objects & equipment (ie. struck by object/equipment, caught in equipment)
c.) Slips, trips, and falls (i.e. falling to a lower level)
Many of these injuries result in pain to the injured worker. Those suffering such injuries will usually meet recovery standards, regrettably others may experience pain that lasts for months, if not years. These patients that endure longer-term pain are categorized as the one out of every six (iii) Americans with chronic pain.
Definitions of chronic pain can vary amongst the medical community. Most practitioners generally view chronic pain as pain lasting three months (iv) or more (v) . Chronic pain holds a wide range of conditions, with spouts of pain staying as little as three months to indefinitely. Intractable pain is on the more severe side of the chronic pain spectrum. The condition of intractable pain is considered pain that is not only chronic but unresponsive to traditional treatment. As the subject of intractable pain continues to be comprehensively reviewed states have taken on different definitions. It is suggested that high-impact chronic pain including intractable pain affects 7.4 percent (vi) of the population with varying severities and is associated more with Americans who live in more rural areas.
With the field of pain management expanding to new therapies, injured workers today have more options at their disposal than ever before. Experimentation such as the emergence of stem cell therapy (vii) is pushing the boundaries of pain management study with novel techniques in treatment being developed and perfected. Although, until these innovations make their way through proper channels and federal clinical clearance, injured workers will have little choice but depend on mainstream routes to cope with their pain.
SHIFTS IN WORKERS' COMPENSATION PAIN MANAGEMENT
Analyzing claims from 2018 through 2021, dermatological agents such as topicals (creams, gels ointments) comprised on average, 20 percent of a state's workers' compensation prescription payments, the highest of all drug categories. Meanwhile, NSAIDs made up around 18 (viii) percent of all prescription payments on average. In states such as California NSAIDs were more than one-third (ix) of all drugs dispensed. Meanwhile anticonvulsants, such as gabapentin, encompassed approximately ten percent of a state's prescription payments. From 2015 to the first quarter of 2021, topicals saw a 10 point uptick (x) in payment share, indicating the possibility of greater use of dermatological agents in workers' compensation. The same trend can be witnessed NSAIDs with more moderate increases.
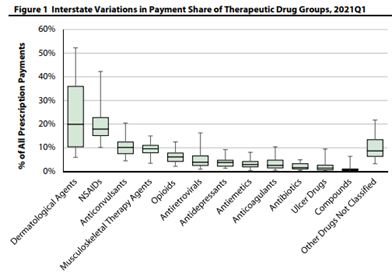
Workers' Compensation Research Institute (WCRI) June 2022
Medical Cannabis
Medical cannabis is also an option for those struggling with mainstream approaches. The substance shows improvement in a variety of pain symptoms. In addition, a peer-reviewed University of Michigan study (xi) revealed a 64 percent reduction in opioid use amongst chronic pain patients utilizing medical marijuana. Multiple studies have demonstrated a variety of positive developments in pain patients who use medical cannabis. Cancer patients and those undergoing chemotherapy, in particular, have seen significant improvements in symptom relief of 30 percent (xii) or more. Currently, the U.S. Food & Drug Administration gives its seal of approval to one cannabis-derived drug and three cannabis-related drug products, showing that cannabis-based treatments will likely play a future role in pain management.
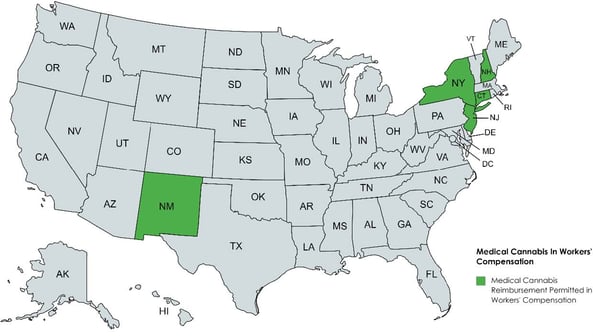
While medical marijuana is somewhat effective in mitigating the pain of those with certain chronic illnesses and cancer, it is clinically less helpful (xiii) in treating acute pain, seizures, and certain inflammatory diseases. According to available studies, the plant-derived substance is shown only to treat certain conditions. There is also a plethora of regulatory and clinical (xiv) roadblocks to medical cannabis. As the substance is still considered a Schedule I drug under the Controlled Substances Act (CSA), several providers are cautious about prescribing medical cannabis in workers' compensation. For those practitioners who recommend medical cannabis, reimbursement from a workers' compensation carrier for such treatment is an obstacle. Despite most states having medical marijuana programs in place and an increased number of states fully legalizing recreational use, only a handful of states allow reimbursement of medical cannabis for workers' compensation injuries, such as Connecticut, New Hampshire, New Jersey, New Mexico, and New York. The U.S. Supreme Court's decision not to hear the issue, signals that individual states will continue to take their own approach to reimbursement of medical cannabis in workers' compensation.
The rise in non-opioid medications and treatment options come at the same time opioid use, and payments are significantly declining in workers' compensation. The Center for Disease Control (CDC) reports that workers' compensation claims with at least one prescription for opioids have witnessed a 55 percent decline (xv) since 2012. Since 2018 per claim payments for opioids have decreased by 56 percent (viii) in the typical state.
Nonpharmacologic options, such as physical therapy, do provide another avenue for injured workers to explore. Some of those hurt on the job may even use physical therapy in conjunction with prescribed medicines to speed up or enhance recovery. However, timing is vital for injured workers if choosing physical therapy (PT). The Workers' Compensation Research Institute (WCRI) indicates that those starting PT early in their injury have better general outcomes and quicker recoveries. In contrast, the institute found that weeks of temporary disability per claim were 58 percent (xvi) longer for those commencing PT 30 days or more after injury. Overall, PT is shown to improve (xvii) recovery and shorten temporary disability duration if treatment begins quickly after injury. Unfortunately, a workers' compensation claim, more often than not, will take time, lessening the chance of starting proper PT services within 30 days of the post-injury timeline.
A new shift to non-opioid alternatives and non-pharmacological options is steadily becoming the norm in workers' compensation. This progression shows the industry's willingness to evolve and provide increased opportunities to care for injured workers in their quality of care.
ADDRESSING THE NEEDS OF CHRONIC & INTRACTABLE PAIN PATIENTS
Promising modernized therapies and alternatives are slowly but surely making their way to the mainstream in years to come. Until then, pain management advocates say chronic and intractable pain patients are at the present moment, left with little relief for their pain. For some dealing with chronic and intractable pain, who have attempted numerous therapies without success, clinically supervised opioid therapy may be the only path to find some reprieve from their pain symptoms. However, numerous injured workers dealing with chronic pain struggle to gain access to such medications that allow them to function for daily activities and provide some type of normalcy.
Center for Disease Control (CDC) guidelines released in 2016 (xviii), while well-intentioned to reduce opioid prescribing to the general population, have adversely impacted chronic and intractable pain patients access. The guidelines called for stringent limits on opioid access, dosage, and even tapering. Such constraints have created a sense of fear for prescribers and heightened liability, producing a clinical environment inhospitable to chronic pain patients, leaving many to deal with their pain among limited resources.
Despite good faith efforts to get a hold of the opioid crisis by regulators, the guidance inadvertently punished those who found opioid treatment as one of their only solutions to managing pain. Ridden with daily chronic pain, many have seen their treatments disrupted and filled with obstacles, only delaying care. The National Pain Advocacy Center warns that more than 50 percent (xix) of doctor’s won’t see a patient who manages pain using opioids and 81 percent were “reluctant” to. A 2018 American Cancer Society research poll found that due to restrictive opioid measures, 56 percent (xx) of patients with serious illnesses said their doctor indicated that treatment options were limited by laws, guidelines, or insurance coverage exclusions. Over a quarter (xx) of American cancer patients and survivors acknowledged that they could not receive an opioid prescription for their pain because a pharmacist refused to fill it. Similarly, over 30 percent (xx) of cancer patients and survivors experiencing chronic pain could not receive opioid medicine as their insurance plan refused to cover it. The swift changes to the prescribing guidelines also posed a threat to patients with sudden tapering, as those cut off from opioid pain management were left with potential physical and mental agony resulting in a heightened risk of suicide (xxi). A number of experts (xxii) believe the protocols also allowed insurers to force changes in care that were not clinically safe for pain patients.
It is estimated that since the 2016 CDC guidelines were issued, most states altered their prescribing laws. Approximately 40 states (xxiii) enacted laws that limit the length of initial opioid restrictions, and 11 states have statutes capping the daily allowable dose. Most state implementing these laws did permit for exceptions particularly for those with cancer and palliative care. Despite several exceptions for certain conditions those with chronic or intractable levels of pain without an oncology diagnosis or specified disease were left with limited exceptions. Even among states attempting to address such high levels of pain with exceptions, the 2016 guidelines continue to deter practitioners from engaging in the treatment of these patients.
In 2019, the CDC acknowledged (xxiv) that some policies and practices attributed to the initial guidelines were inconsistent with its recommendations. Rather than be an intended roadmap for clinicians navigating the complexities of pain management, the guidance measures were misapplied and improperly considered a set of rigid rules, according to federal officials. To rectify circumstances, the Center put forth newly proposed guidance in 2022 that would enable better access for those facing chronic and intractable pain, emphasizing individualized patient-centered decision-making. The proposal from the agency no longer lists specific limits on the dose/duration of an opioid prescription and promotes a best judgment practices approach among clinicians. This move is seen by pain management advocates as a step in the right direction and should be worth closely monitoring by stakeholders as it makes its way through the rules process.
STATE ACTIONS
2018 Pain Policy in the States
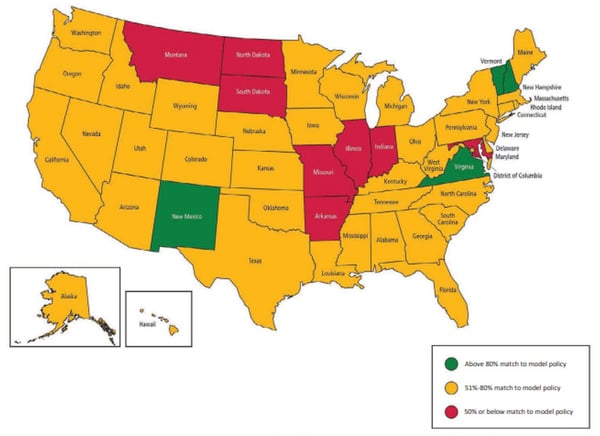
American Cancer Society Pain state rankings in accordance with access, regulation, and attention to patient's pain needs.
Most states and their agencies require the treatment of those going outside of traditional opioid guidance to be documented, tracked, and closely monitored by a physician. To help pain management patients attain access to their medical needs, several states have passed legislation at the state level. In 2022 alone, Arizona, Oklahoma, and Rhode Island took comprehensive steps to ensure those with chronic pain could receive and seek out appropriate treatments.